Evaluation of the colorectal cancer screening program in the Czech Republic
Monika Ambrožová1,2, Petr Dvořák1, Renata Chloupková1,2, Ondřej Ngo1,2, Veronika Rybenská1, Karel Hejduk2,1, Ladislav Dušek Orcid.org 1,2, Ondřej Májek Orcid.org 2,1
+ Affiliation
Summary
Introduction: Colorectal cancer (CRC) screening is a key tool for secondary prevention, whose effectiveness depends on population participation, accessibility of care, and quality of the examinations. Its impact is further determined by systematic data collection and analysis. High-quality data represent a fundamental pillar for monitoring ongoing screening, evaluating outcomes, and identifying weaknesses in the program. The aim is to demonstrate the benefits of data for optimizing the Czech program through two case studies. Methods: Data sources included the National Health Information System and the Database of Preventive Colonoscopies managed by the Institute of Health Information and Statistics of the Czech Republic, complemented with sociodemographic data from the Czech Statistical Office. Evaluation was carried out using screening quality indicators and a budget impact analysis focused on the change of age limits in screening. Results: The first case study shows a 33% decrease in CRC incidence and a 49% reduction in mortality since program implementation. Coverage of the target population has long remained around 30%. In 2020, a positive fecal occult blood test (FOBT) rose to 10%. The interval between a positive FOBT and follow-up colonoscopy corresponds to 3 months. The uptake of follow-up colonoscopy after a positive FOBT reaches 60%. The second case study revealed that expanding the eligible age range from 45–74 years will initially lead to a 5–6% increase in costs; however, from 2029 onwards, a reduction is expected. Discussion: The first study demonstrates the success of screening in reducing incidence and mortality, while also highlighting challenges such as low coverage, high FOBT positives, long waiting times for follow-up colonoscopy, and low uptake of follow-up colonoscopy. The second study found that expanding the age range will be cost-effective. Data confirm the benefits of screening for population health and indicate areas requiring further attention. Conclusion: Systematically collected and analyzed data are an essential component for evaluating and managing screening programs. The case studies illustrate their applicability in monitoring care quality and supporting health policy decisions.
Keywords
colorectal cancer, screening, colonoscopy, occult blood, adenoma, quality indicators, data, statistical analysis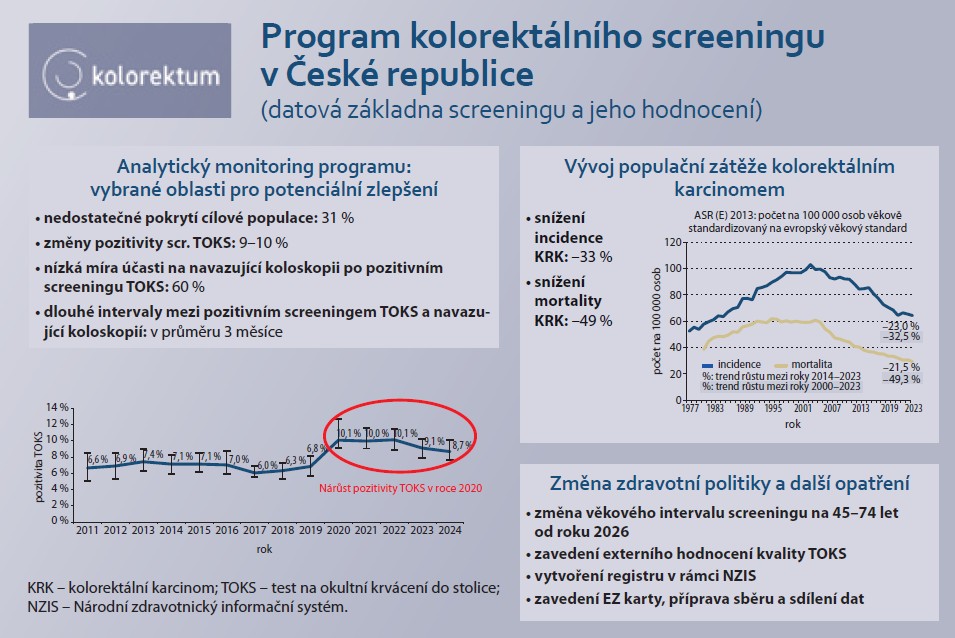
To read this article in full, please register for free on this website.
Benefits for subscribers
Benefits for logged users
Literature
1. MZČR. Standard při poskytování a vykazování výkonů screeningu nádorů kolorekta v České republice. 2024 [online]. Dostupné z: https://www.kolorektum.cz/res/file/legislativa/vestnik-01-09-crca.pdf.
2. Hejduk K, Mandelová L, Ngo O et al. Národní screeningové centrum. 2024 [online]. Dostupné z: https://www.uzis.cz/index.php?pg=centra--nsc.
3. Chloupková R, Benáček P, Ngo O et al. Národní screeningové centrum: datový portál screeningových programů. 2022 [online]. Dostupné z: https://nsc-data.uzis.cz/.
4. NZIP. Národní zdravotnický informační portál. 2025 [online]. Dostupné z: https://www.nzip.cz.
5. SVOD. Portál epidemiologie novotvarů v ČR. 2024 [online]. Dostupné z: https://www.svod.cz.
6. MZČR. Zápis z jednání Komise pro program screeningu kolorektálního karcinomu. 2025 [online]. Dostupné z: https://ppo.mzcr.cz/upload/files/zapisy-z-jednani-komise-krk-zapis-28-4-2025-683947a0483ad.pdf.
7. NSC. Program screeningu kolorektálního karcinomu. 2025 [online]. Dostupné z: https://www.kolorektum.cz.
8. Karsa L, Patnick J, Segnan N. European guidelines for quality assurance in colorectal cancer screening and diagnosis. 2010 [online]. Dostupné z: https: //data.europa.eu/doi/10.2772/1458.
9. MZČR. Oznámení ve věci úpravy Věstníku MZ ČR částka 1/2009 Standard při poskytování a vykazování screeningu nádorů kolorekta. 2023 [online]. Dostupné z: https: //mzd.gov.cz/oznameni-ve-veci-upravy-vestniku-mz-cr-castka-1-2009-standard-pri-poskytovani-a-vykazovani-screeningu-nadoru- kolorekta/.
10. Milcamps A, Alexandru A, Baldacchino S et al. Uncovering inequalities: colorectal cancer screening in Europe. 2024 [online]. Dostupné z: https: //publications.jrc.ec.europa.eu/repository/handle/JRC137531.
11. Gartlehner G, Schernhammer E, Lax SF et al. Screening for colorectal cancer: a recommendation statement of the Austrian National Committee for Cancer Screening. Wien Klin Wochenschr 2023; 135(17–18): 447–455. doi: 10.1007/s00508-023-02209-0.
12. Penz D, Waldmann E, Hackl M et al. Colorectal cancer and precursor lesion prevalence in adults younger than 50 years without symptoms. JAMA Netw Open 2023; 6(12): e2334757. doi: 10.1001/jamanetworkopen.2023. 34757.
13. Jahn B, Sroczynski G, Bundo M et al. Effectiveness, benefit harm and cost effectiveness of colorectal cancer screening in Austria. BMC Gastroenterol 2019; 19(1): 209. doi: 10.1186/s12876-019-1121-y.
14. Gsur A, Baierl A, Brezina S. Colorectal cancer study of Austria (CORSA): a population-based multicenter study. Biology (Basel) 2021; 10(8): 722. doi: 10.3390/biology10080722.
15. Wolf AM, Fontham ET, Church TR et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin 2018; 68(4): 250–281. doi: 10.3322/caac.21457.
16. Dangi-Grimella S. USPSTF: screening for colorectal cancer should start at 45. 2024 [online]. Dostupné z: https: //coloncancerfoundation.org/uspstf-screening-for-colorectal-cancer-should-start-at-45/.
17. Shaukat A, Kahi CJ, Burke CA et al. ACG clinical guidelines: colorectal cancer screening 2021. Am J Gastroenterol 2021; 116(3): 458–479. doi: 10.14309/ajg.0000000000001122.
18. Patel SG, May FP, Anderson JC et al. Updates on age to start and stop colorectal cancer screening: recommendations from the U.S. multi-society task force on colorectal cancer. Gastroenterology 2022; 162(1): 285–299. doi: 10.1053/j.gastro.2021.10.007.
19. Karsenti D, Tharsis G, Burtin P et al. Adenoma and advanced neoplasia detection rates increase from 45 years of age. World J Gastroenterol 2019; 25(4): 447–456. doi: 10.3748/wjg.v25.i4.447.
20. Mitsuhashi S, Azari J, Dioguardi V et al. Age matters: adenoma detection rates in average-risk screening patients aged 45 to 49 compared with those aged 50 to 54. J Clin Gastroenterol 2024; 58(9): 896–901. doi: 10.1097/MCG.0000 000000001953.
21. Bilal M, Holub J, Greenwald D et al. Adenoma detection rates in 45–49-year-old persons undergoing screening colonoscopy: analysis from the GIQuIC registry. Am J Gastroenterol 2022; 117(5): 806–808. doi: 10.14309/ajg.00000000000 01684.
22. Ladabaum U, Mannalithara A, Meester RGS et al. Cost-effectiveness and national effects of initiating colorectal cancer screening for average-risk persons at age 45 years instead of 50 years. Gastroenterology 2019; 157(1): 137–148. doi: 10.1053/j.gastro.2019. 03.023.
23. Australian government: department of health, disability and ageing. Lowered eligible age for bowel screening. 2024 [online]. Dostupné z: https: //www.health.gov.au/our-work/national-bowel-cancer-screening-program/about-the-national-bowel-cancer-screening-program/lowered-eligible-age.
24. Lew JB, Worthington J, Ge H et al. Re-evaluating population-level screening recommendations to address increasing early-onset colorectal cancer rates in Australia: a modelling study. ESMO Gastrointest Oncol 2025; 7(6): 100136. doi: 10.1016/j.esmogo.2025. 100136.
25. Currais P, Mão de Ferro S, Areia M et al. Should colorectal cancer screening in Portugal start at the age of 45 years? A cost-utility analysis. GE Port J Gastroenterol 2021; 28(5): 311–318. doi: 10.1159/000513592.